Note: if you are planning a natural birth, especially with hypnosis, don't read this without your "Bubble of Peace" on Mega-Force-Field-Strength. If you are planning a peaceful, wonderful, pleasant and awesome birth and you want to visualize only wonderful happy things, click here for my favorite water birth video.
If you'd like to learn about real medical reasons for c-sections so you can potentially help avoid an unnecessary one, please proceed.
You've been warned. Bubble up?
Necesareans

The current US c-section rate is somewhere between 33 and 38% of all deliveries. The World Health Organization states that no region in the world should have a rate greater than 10-15%. If the WHO is correct, that means that 54%-73% of all American cesarean deliveries are unnecessary. Average the numbers out, and that means that 2 out of every 3 c-sections performed in the USA may be unnecessary. Let’s play with some pretend, averaged and hypothetical numbers.
 |
| The 2010 rate is estimated at 33.9%. |
100 laboring women. 33 have c-sections. 22 women had surgery they may have been able to avoid.
Now here’s the twist. 11 of them did need c-sections. There are valid medical reasons for c-sections. Women used to die in labor, far more often than they do today. Babies used to die in horrific numbers during childbirth, and the c-section is an amazing medical advance, a relatively “safe-ish” surgery that can and does save lives. Before the advent of the c-section, labor and delivery were leading causes of death for young women and babies. Since 1980 (and not on this chart), the number of maternal deaths is rising again, and many say it is because of the overuse of the cesarean section.
 |
| Maternal deaths per 100,000, 1880-1980 |
How do you know which one you are? Is your birth a real emergency, one of the 11, or one of the 22 that might have been avoided and could be putting you and your baby at needless risk? Your doctor will always tell you that you’re one of the 11, unless you have an elective surgery (very rare – despite the hype, less than 0.5% of c-sections are truly elective, with zero “medical” reasoning provided). Your doctor will always say that you had a c-section because it was necessary.
So, you’re in labor, or close to it. Things aren’t going according to plan. Your doctor wants to do a c-section, and they’ve been to medical school. You haven’t. How do you keep from being part of the 22? How do you know if you’re one of the 11? Ultimately, you have to trust your care provider, which is why selecting one is so very important. You also have to do everything you can to reduce your risk of running into a real medical reason (avoiding interventions unless they are medically necessary).
Below is a list of medical indications for cesarean section, with details. Knowledge is power, right?
As always, please note: I am not a doctor. I have not gone to medical school. I have never performed a c-section. I am not an expert. I am a mommy who likes to write stuff and post it on the internet. Please do not take anything I write as medical advice, but as information and opinion. Inform yourself, do your own research, and talk to your medical experts before you make a serious decision that could seriously impact you and your baby.
Necessary C-Sections
Placenta Previa
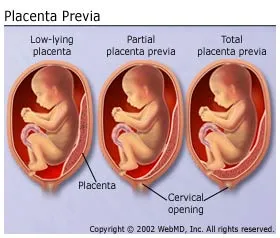
Placenta Previa means that your placenta is located above your cervix. Both partial and complete placenta previa (placenta blocks the cervix completely at the time of delivery) is absolutely an indication for c-section. If your placenta blocks your baby’s exit, you are at risk for extreme bleeding, and there is no way for the baby to get out.
What you should know: Placentas can move. Suspected placenta previa can be often be confirmed via ultrasound or even via vaginal exam. Just because you have a low-lying placenta early in your pregnancy does not mean it won’t shift out of the way by the time of delivery. “Marginal” placenta previa, where the placenta is just very close to the cervix, is not generally an indication for c-section. You should know which one you have before you consent; information is power.
Cord Prolapse

If your water breaks, and the cord comes out before the baby, this is Umbilical Cord Prolapse. Cord prolapse is an immediate emergency – either you must immediately deliver vaginally, or proceed directly to the OR. Time is of the essence to save the baby’s life – whichever method gets the baby out fastest should be used.
What you should know: Cord prolapse is much more likely to happen if your baby is premature, and especially if your waters are broken artificially. So, if your care provider offers to "get things moving" by breaking your water with a hook, remember that this is a (small) possibility.
“True” Knot in Umbilical Cord

These are very difficult to diagnose prenatally, but it has happened with 3D ultrasound (which carries risk). A true knot is exactly what it sounds like - it can prevent oxygen from getting to the baby. If one is seen on ultrasound (again, rare – usually they are discovered after delivery), you will likely be sent to the OR.
Placental Abruption

If your placenta detaches from the wall of your uterus while the baby is still inside you, this is a placental abruption. Symptoms are severe abdominal pain, heavy bleeding and back pain. Partial abruption prior to labor is usually treated by bed rest and transfusions, but a complete abruption at any point or any kind of abruption during labor is an emergency situation. Like a cord prolapse, immediate steps need to be taken to get the baby out – immediate vaginal delivery or emergency cesarean.
Click here to read a very sad story about a baby lost due to an abruption - recognizing the symptoms of an abruption and seeking immediate, emergency help is vital to avoiding this tragic result.
Click here to read a very sad story about a baby lost due to an abruption - recognizing the symptoms of an abruption and seeking immediate, emergency help is vital to avoiding this tragic result.
Uterine Rupture
If the uterus tears, an immediate, emergency c-section must be performed to save the life of the mother and baby. This is rare (1/1500 births).
What you should know: Risk of uterine rupture is often given as a reason not to allow VBACs (vaginal birth after cesarean). New research shows that the risk of c-sections may be higher than the risk of rupture, which is very rare.
Toxemia, Severe Pre-Eclampsia, HELLP syndrome, pregnancy-induced hypertension

Pregnancy-induced hypertension is high blood pressure that just keeps rising. Eclampsia, toxemia and HELLP are all potential complications of uncontrolled high blood pressure in a pregnant woman. If PiH isn’t controlled, high blood pressure can cause strokes, cerebral hemorrhage, respiratory distress and even death for the mother, as well as endanger the baby. Toxemia, HELLP and Eclampsia are all potentially deadly complications of uncontrolled PiH.
During pregnancy, there are a number of treatments that can slow disease progression. The only “cure” is delivery. If your blood pressure rises severely enough and quickly enough, it is imperative to get the baby out ASAP. BP over 160/110 is considered severe. Because prolonged labor can be stressful on your body (not that c-sections aren’t!) many doctors prefer to perform a c-section to avoid the possibility of your blood pressure rising further. If the situation becomes unmanageable, immediate action to deliver the baby is required.
You should know: You can reduce the risk of pre-eclampsia with diet and exercise, among other things. Click here for more information about pre-e (to start).
Transverse Lie (baby is lying sideways)
While it is possible to deliver a breech baby vaginally, it is not possible to deliver a baby who is sideways in the womb. That being said, babies move. Just because your baby is sideways NOW doesn’t mean they’ll be sideways when you actually go into labor. 80% of babies who are transverse at 37 weeks have moved when you go into labor! So, don’t just schedule the c-section. Wait to see if baby flips. Check out http://www.spinningbabies.com/ if you want to get your baby on the move.
You should know: While transverse lie is an indication for surgery, breech often isn't. See below.
Acute Fetal Distress

Fetal distress is often used as a reason for c-section delivery, but the definition is nebulous. “We’re worried about the baby” is a sure-fire way to get a laboring woman into the OR without argument. There is a difference between “fetal distress” and “acute fetal distress.” There is a clear definition of acute fetal distress.
Most babies become mildly distressed during labor – so do many moms! Being born is hard work, and it can be stressful. Your baby is often working as hard as you are in this team effort. There’s a BIG difference between being stressed and being in danger. Below are the textbook definitions of “Acute Fetal Distress”. #1, 2 and 5 alone are enough to indicate acute distress. #3 and 4 are used in conjunction with other factors.
1 – Fetal heart rate greater than180 bpm or less than 100 bpm for longer than 4 minutes. Note – an occasional rise or fall to these numbers does not automatically indicate distress. An average over one minute is used.
2- Repeated or variable deceleration. It is normal for the baby’s heart rate to increase and decrease during and after contractions. If the dips become too severe, it can indicate fetal distress. If they don’t happen in time with the contractions (variable), they could be related to something else, such as trouble with the cord or placenta.
3 – Meconium staining of the amniotic fluid. This alone is not necessarily an indication of distress, but it is a symptom. Distressed babies release meconium (poop in the womb). Not all babies who produce meconium in utero are distressed. (Irish girls have pale skin. Not all girls with pale skin are Irish.)
4 – Fetal Movement: frequent decrease and weakening. Again, this is not an indicator by itself; many babies get “quiet” during labor, often just to sleep. If decreased movement happens along with another factor, it’s cause for concern.
5 – Acidosis: If you want to be sure if your baby is in distress and there is time, this is a definitive test. A blood sample is taken from your baby’s head (a tiny scratch). They can immediately test the blood’s PH, oxygen and carbon dioxide levels to see if your baby isn’t getting enough oxygen. This is only possible if the baby’s head is engaged and your water had broken.
pH below 7.20 (Additional information about acidocis here)
pO2 (oxygen level) below 10mmHg
CO2 (carbon dioxide) above 60mmHg
If the baby is in acute distress, it’s time to get the baby out, by the swiftest method possible. Please, if your doctor says the baby is in danger, don't spend time printing out this post and checking the lab work...
More information about fetal distress here
More information about fetal distress here
You should know: If the baby is in mild distress, the first course of action should be to attempt to remove whatever is causing distress. Sometimes, your position can be compressing the cord – occasionally, if you change position (lie on your side, your stomach, or even get in a tub), this can alleviate pressure and allow the cord blood to flow properly. If you’re on pitocin, they should turn it off. Overly strong contractions can stress the baby.
Previous Abdominal Surgery
This is not absolute, but depends on the type of incision and the type of scarring. Certain abdominal surgeries can cause complications during vaginal childbirth. One example is a iliostomy/j-pouch surgery, removal of intestines, vertical previous c-section, or c-section that is not yet healed (less than 1 year). Necessity is dependent on the location of scarring and weaker tissue.
Active Herpes Lesions
If you have genital herpes and have active lesions, you can pass the disease on to your baby at birth. Herpes can be deadly to a newborn, and there is no cure, so they’ve got it for life. Between 10 and 14% of women with genital herpes have a lesion at delivery. The chance of passing the virus to your baby decreases based on the amount of time Mom has had the disease. If you have had herpes for years, the theory goes that you have developed antibodies and will pass these to your baby – even if you have a current lesion. If you acquire herpes during your pregnancy, especially during the 2nd and 3rd trimester, your risk is highest, and you may consider a c-section even if no lesions are present. See this site.
Multiples greater than twins

Triplet and higher deliveries are almost always delivered by c-section. First, these deliveries are rarely full-term, and premature babies may not handle the stress of labor as well as full-term babies. Second, 3+ cords and 3+ placentas can be complicated.
You should know: Twins are regularly delivered vaginally without complication. Even triplets can and have been delivered vaginally (see here for a recent study), but this is rare because triplets and greater so often arrive ahead of schedule.
Known Health Emergency for Baby
If your baby has certain known health issues or birth defects (I hate that phrase, no baby is “defective”) that need to be addressed immediately, a cesarean section may be your best choice. Work with your neonatologist.
Health of the Mother
If a mother is physically incapable of labor because of her own health conditions, c-section is the alternative. Some examples include physical abnormality (certain kinds of dwarfism or pelvic abnormalities), some kinds of paralyzation, out-of-control diabetes, and a few other extreme conditions.
Generally speaking, most women are capable of at least attempting a vaginal birth (there is stress involved in a c-section as well; delivering a baby isn't a walk in the park no matter what your health). You and your doctor need to weigh the benefits and risks.
DEBATED REASONS
These are reasons often given for cesarean sections. There is debate about them. Some people say they’re necessary to mitigate risk, others say that vaginal birth should first be attempted. Do your research, work with your care providers and reach your own conclusions.
If you do decide to have a c-section, armed with the facts, more power to you. My goal is informed consent. If you personally decide that the risks of a c-section are less than the risks of vaginal birth, awesome. I just hate to see women pressured into something they "had" to do when they didn't want it.
Abnormal Fetal Position (breech):

Most midwives and doctors will not deliver a breech baby vaginally – but some will. Many babies are born happily and peacefully in the “frank breech” position, that is, butt first, feet by head. This position is most favorable to vaginal birth, if you can find an experienced provider who is willing to assist. Breech babies have all been delivered successfully vaginally. Breech births do carry higher risks of cord prolapse, increasing with the type of breech delivery. Not included here is Footling breech, which carries the highest risk. In this presentation, baby comes out feet first.
If you attempt vaginal delivery of a breech baby, it is of vital importance that your midwife/OB be well-versed in the intricacies of breech birth. If you can’t find one (providers are much more rare than breech presentations), you may have a c-section. It is important to note that vaginal breech birth should not be attempted without an experienced medical professional who is on board with delivering breech. There are risks to delivering breech vaginally; neonatal death has happened as a result of breach deliveries being handled improperly. Work with your provider to assess your individual situation.
HIV Infection

Some research has shown that HIV transmission from mother to baby can be reduced by surgical delivery. Other research has contradicted this, and found that there is no increased risk with vaginal delivery. For more information, start here and keep on going: http://www.wdxcyber.com/npreg13.htm
Failure to Progress

I would personally argue with this reason. If failure to progress exists but is not accompanied by any health issues for mom or baby (see Acute Fetal Distress above), what most mothers need is patience, not surgery. Mom may need more support. She may need help feeling safe. She may need (eek, omg, yes I’m saying it), help with pain so she can sleep, or other medical assistance. Surgery should be the last option, not the first. Get in a tub. Close the doors and kick the world outside. Listen to soft music, turn down the lights. Magic can happen!
Long ago in caveman days, you wouldn't want to deliver a baby in "unsafe" conditions. Say, there's a warring tribe attacking your cave, or a tiger on the loose - real, physical danger. You wouldn't want to deliver a helpless baby. We're programmed so that labor slows down in periods of stress and fear. Many women who aren't progressing need to feel extra safe and protected before their bodies will allow them to birth their children. Threatening most women with unwanted surgery is not a way to make them feel safe!
Healthy labors can last for days, especially the first time around. This is not necessarily pathogenic. It is annoying to hospital administrations who may want the room for the next woman.... So, personally, unless fetal or maternal health shows signs of deterioration, I'd argue against the knife.
True “failure to progress” is defined as 4 or more hours with no dilation progress, when mom is dilated at least 5cm. Early labor (less than 5cm dilated) can last for a really long time under totally normal circumstances.
Twins (or sometimes even triplets)
Twins are, like breech, a variation on normal. Like breech delivery, you will need to find an experienced caregiver to work with you, but it's absolutely possible. Baby position is also key here - ideal presentation is below, but babies have been successfully delivered in all sorts of presentations.
This is a great site to see videos of twins born vaginally: http://www.givingbirthnaturally.com/natural-childbirth-video.html
This is also a great discussion of mothers who've done it.
An additional complication to the births of multiples is prematurity or babies who are small for their gestational age. Please work closely with a trusted professional to determine your best
An additional complication to the births of multiples is prematurity or babies who are small for their gestational age. Please work closely with a trusted professional to determine your best
 | |
| Twins, both head down, an ideal position for vaginal birth. |
What you should know: Delivering one twin vaginally and then the next by c-section is not unheard of. Some providers (but not all) prefer that you have an OR on "standby" or at least nearby when delivering twins or triplets the old-fashioned way.
Previous Cesarean Delivery
VBACs are not permitted in many hospitals. Why? Well, there have been some studies done that showed an increased risk of uterine rupture in mothers who had previously had a c-section. It scared hospital administrations, and nowadays a lot of hospitals won't let you try vaginally.
The evidence does not support this fear. The risks of a second c-section are usually higher than the risks of attempting vaginal birth. You may have to fight hard for a VBAC, but the evidence is with you.
I am oversimplifying the situations surrounding VBAC - but if you'd like to consider it, please do some research. Not all cesareans are alike, and not everyone is a good candidate for VBAC. If you are a candidate, you may want to consider it. See the bottom of this page for additional information.
I am oversimplifying the situations surrounding VBAC - but if you'd like to consider it, please do some research. Not all cesareans are alike, and not everyone is a good candidate for VBAC. If you are a candidate, you may want to consider it. See the bottom of this page for additional information.
Macrosomia (baby's too big)
This one's tossed around a lot as a reason for surgery. Again, most evidence does not support it.
 |
| I don't remember where I found this picture. |
1 - It is very difficult to truly assess the size of a baby before he's born. Ultrasounds and belly measurements are notorious for being way off.
2 - Most mothers' bodies won't make a baby too big to come out.
3 - Big babies are delivered vaginally all the time. 11-12 pounders!
4 - Baby fat squishes.
If a baby is truly too big to come out the old-fashioned way, that will prove out in labor.
Cephalopelvic disproportion (CPD)
A variation on the "baby's too big" theme, true CPD is also rare, and virtually impossible to diagnose prenatally. CPD means the baby is too large to fit. Sometimes smaller-statured mothers are given this as a reason for c-section.
Tiny mommies have big babies naturally all the time. CPD is real, but it varies widely. Mothers who have had c-sections for CPD have gone on to have successful VBACs.
You should know: If a baby does get "stuck" (shoulder dystocia), changing positions can enlarge the pelvic opening. The Gaskin Manuver is a potentially life-saving technique that can be used in the event of shoulder distocia. The lithotomy position (on your back with your legs up in stirrups) is the one of the *smallest* positions for a woman's pelvis. Flip to all fours or squat, and you can get up to another 3cm in diameter! Shoulder dystocia is a true emergency for the baby, and a competent provider is absolutely essential to saving the baby's life.
Plus-Sized Mama

I am a plus sized mama. I gave birth (vaginally) to a 7 pound baby, who ultrasound "estimated" at 9 pounds 3 days before his birth. Whoops. So much for that "big baby" worry. Some doctors offices will label you "high risk" by the size of clothes you're wearing, and automatically steer your chubby self to the operating table. I call bullsh!t on this one, with some exception.
Generally speaking, if you are healthy enough to vigorously engage in the activity that got you pregnant in the first place, there's no reason that you shouldn't at least attempt a vaginal birth. If, however, you have a hard time getting around, you might have a tough time managing labor. You never know though - you may be surprised with the amazing things your body can do.
In fact, the risks of c-sections are often higher in obese women then the risks of vaginal delivery. Check this out if you're a plus-sized mama-to-be. Personally, I don't see harm in attempting a vaginal birth, no matter what your size - but, again, not a doctor.
You should know: Taking care of yourself during pregnancy and having a supportive care provider are the best ways to ensure a healthy labor and delivery, regardless of your size. If you are plus sized and suspect that your provider is not "size-friendly", switch.

There are undoubtedly many reasons I missed that are either real or dubious reasons for c-section. If you know of any, please comment with them and I will happily edit this article. I will also happily correct any (verifiable) mistakes; I'm not a doctor and I don't play one on the internet.
Ultimately, many c-sections are necessary, but not all of them. Women who have c-sections are no less strong and awesome than those who deliver vaginally, with or without medical assistance. C-sections are not a failure, often they are a massive and amazing miracle that could have resulted in the death of mother or baby not long ago in our history.
What's important through the whole process is informed consent; if you have a c-section, that you understand why it is necessary and agree with your doctors about the choice. Choice, and understanding. C-sections are a blessing and a curse; if used when necessary, c-sections save lives. If unnecessary, they put the health of the mother and baby at increased risk for infection, bleeding, and even death.
What's important through the whole process is informed consent; if you have a c-section, that you understand why it is necessary and agree with your doctors about the choice. Choice, and understanding. C-sections are a blessing and a curse; if used when necessary, c-sections save lives. If unnecessary, they put the health of the mother and baby at increased risk for infection, bleeding, and even death.
Women are people worthy of respect throughout all of labor and delivery. Contrary to media portrayals, we are capable, intelligent and rational people, even after our water breaks. :) We want what is best for our babies, and we want to be treated as adults and active participants in our own healthcare.
Additional Resources:
For more information about the unnecessary c-section epidemic and how it's affecting maternal and neonatal health, check out: http://www.theunnecesarean.com/ and http://www.ican-online.org/
For information about VBACs, click here: http://www.vbac.com/ and http://vbacfacts.com/
For support dealing with birth trauma, including PTSD, visit these sites: http://www.solaceformothers.org/ and http://www.birthtraumaassociation.org.uk/
To learn more about recovering from a c-section, see here: http://www.csectionrecovery.com/ and http://www.csectionguide.com/
Additional Resources:
For more information about the unnecessary c-section epidemic and how it's affecting maternal and neonatal health, check out: http://www.theunnecesarean.com/ and http://www.ican-online.org/
For information about VBACs, click here: http://www.vbac.com/ and http://vbacfacts.com/
For support dealing with birth trauma, including PTSD, visit these sites: http://www.solaceformothers.org/ and http://www.birthtraumaassociation.org.uk/
To learn more about recovering from a c-section, see here: http://www.csectionrecovery.com/ and http://www.csectionguide.com/













{kind=link}
{kind=link}